- LOGIN
- MemberShip
- 2026-06-11 09:26:14
- Policy
- Stepwise price reduction applied from 13th listed product
- by Jung, Heung-Jun Mar 16, 2026 09:25am
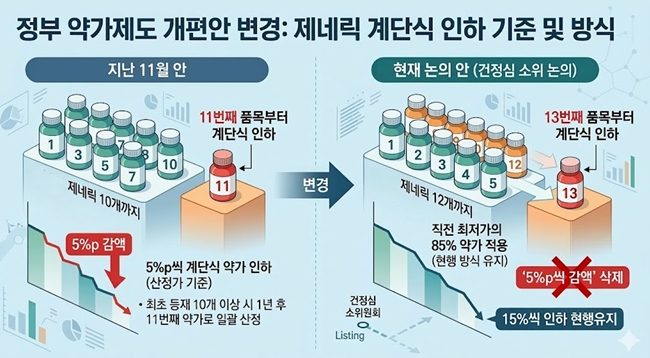
- The government, which had planned to implement stepwise drug price reductions of 5 percentage points starting from the 11th listed product, has decided to revise both the criteria for listing items and the reduction method.The new direction under discussion is to apply stepwise reductions starting from the 13th listed product, while maintaining the current method of applying 85% of the previous lowest price as the new price.According to industry sources on the 16th, the government’s drug pricing system reform proposal discussed at the recent Health Insurance Policy Deliberation Committee (HIPDC) subcommittee differs from the proposal announced in November last year.The stepwise drug price reduction reform plan is expected to undergo partial changes. AI-generated imageThe reform plan from last November included a method whereby “the price of the first generic would be reduced by 5 percentage points starting from the 11th product listing of the same formulation.” This represented a significant strengthening of the current product reduction system, which is applied starting from the 21st listed product.Additionally, the plan stipulated that if there were 10 or more initially listed generics, the price would be uniformly set at the 11th product’s level one year later.At this HIPDC subcommittee meeting, a proposal to apply the stepwise reduction starting from the 13th product was discussed. While the method of reducing the price by 5 percentage points each time would be removed, discussions are focused on maintaining the approach of applying a price set at 85% of the lowest price for subsequent listings. This effectively means maintaining the current reduction rate of 15% applied from the 21st product onward.Products listed at the point where stepwise reductions begin will have their prices adjusted to 85% of the lowest price after one year.For example, if there were 10 products this month and the number exceeds 13 with next month’s listings, the price for the newly listed products will be set at 85% one year later. However, if additional items are listed the following month, their prices would be further reduced by an additional 85% on top of the 85% already applied.Although the threshold number of products used as the basis for stepwise reductions has been slightly relaxed, the system still effectively results in an additional 15% reduction following the initial 15% reduction, depending on the listing timing.However, the details currently under discussion are not yet finalized. There is a possibility that the application method or specific figures could change at the HIPDC meeting on the 26th.Additionally, since the generic drug pricing rate is not clearly defined as being in the “mid-to-high 40% range,” the exact drug price calculations under stepwise reductions will likely be possible only after the HIPDC decision is finalized.
- Company
- Government sticks to low-40% pricing for generic drugs
- by Kim, Jin-Gu Mar 13, 2026 09:06am
- The government has reportedly decided to maintain its plan to apply a generic drug pricing ratio in the “low to mid-40% range” compared to original drugs. This position remains significantly different from the compromise proposal of about 48% suggested by the pharmaceutical industry, which had already represented a 10% reduction from the current level. Criticism is expected that the government is not demonstrating sufficient willingness to communicate with the pharmaceutical industry regarding drug pricing policy, despite industry objections.According to industry sources on the 11th, the MOHW held a subcommittee meeting of the Health Insurance Policy Deliberation Committee that day to discuss the drug pricing system reform plan. In the closed-door meeting, the MOHW reportedly presented a generic drug pricing calculation rate in the low to mid-40% range.This level is largely consistent with the direction the government presented during last month's HIPDC discussions. Last November, the MOHW reported a drug pricing system reform plan to the HIPDC. This plan included lowering the drug pricing ratio for generics and off-patent drugs from 53.55% to the 40% range.At that time, the ministry indicated that the new generic pricing calculation standard would likely be set between 40% and below 45%. When presenting the reform proposal, the ministry also outlined a schedule for adjusting the prices of already listed drugs. It stated that products currently priced at 45-50% would begin price adjustments in 2027, with reductions to the 40% range by 2029.This still shows a considerable gap from the 48% compromise level proposed by the pharmaceutical industry. The pharmaceutical industry has presented its bottom line for an acceptable calculation rate, signaling its willingness to negotiate with the government.On the 10th, the Emergency Response Committee for Drug Pricing Reform for Pharmaceutical Industry Development held a press conference and proposed joint research with the government, including analysis of price reduction impacts.At the press conference held by the ‘Emergency Response Committee for Drug Pricing Reform for Pharmaceutical Industry Development’ at the Korea Pharmaceutical and Bio-Pharma Manufacturers Association on the 10th, the committee proposed that “considering the profitability of listed pharmaceutical companies and industry conditions, the acceptable price for generic drugs would be about 48.2% of the original drug price.”The specific pricing ratio is expected to be confirmed at the full committee meeting scheduled for the 26th. However, the key question is whether there will be a re-discussion process before the agenda is submitted to the full committee meeting.In this regard, concerns have been raised in the National Assembly that the drug pricing reform plan is being pushed forward without sufficient discussion.Representative Sunmin Kim of the Rebuilding Korea Party pointed out during the National Assembly Health and Welfare Committee plenary meeting on the 10th that the Ministry of Health and Welfare had attempted to ‘pass NA’ by proceeding with the HIPDC subcommittee and plenary meeting schedules in March without including the drug pricing reform plan in its annual report to the National Assembly.Representative Joo-min Park of the Democratic Party of Korea, who chairs the Health and Welfare Committee, agreed that a separate briefing on the reform plan is necessary. He told Health and Welfare Minister Eun-Kyoung Jeong, “Since this is an extremely important matter, it would be appropriate to provide an additional report at the plenary session after discussions on the reform plan are completed.”As a result, the ministry is increasingly likely to provide a separate briefing on the direction of the drug pricing reform plan to the National Assembly before the HIPDC plenary vote.Currently, the MOHW plans to vote on the drug pricing system reform plan at the HIPDC plenary meeting on the 26th. This plan includes lowering the pricing ratio for already-listed generic drugs from the current 53.55% to the 40% range.The generic pricing ratio is the key issue in the current drug pricing reform debate. Currently, domestic generic drug prices are set at 53.55% of the original drug price. The government is pushing to reduce this ratio to the 40% range.In response, the pharmaceutical industry has raised concerns that an excessive price reduction could lead to deteriorating corporate profitability, reduced investment in research and development, and employment instability. As an alternative, the industry proposed a moderated reduction with a pricing ratio of around 48%.
- Company
- New RSV prophylaxis is entering KOR…expanded infant protection
- by Son, Hyung Min Mar 13, 2026 09:06am
- The prevention strategy for infant respiratory syncytial virus (RSV) is expected to expand rapidly in South Korea.As global pharmaceutical companies are proceeding with regulatory approval processes for maternal vaccines and new antibody injectables, a new competitive landscape is beginning to take shape. RSV vaccine 'Abrysvo'According to industry sources on the 13th, Pfizer Korea has summitted application for the approval of 'Abrysvo,' its RSV vaccine. Approval is anticipated within the first half of this year.Abrysvo is a vaccine that targets the F protein, a major surface protein of RSV. It is specifically designed based on the pre-fusion (pre-F) form of the F protein, which the virus uses to penetrate cells.The pre-F protein is known to be the most effective antigen for inducing neutralizing antibodies, as it represents the viral structure just before cell binding and entry. Abrysvo induces an immune response using a protein that stabilizes this specific structure.Designed as a bivalent vaccine targeting both major RSV subtypes (A and B), Abrysvo uses a maternal immunization strategy. In this approach, antibodies generated by the mother following vaccination are transferred through the placenta to protect the infant after birth.RSV is a leading respiratory virus causing pneumonia and bronchiolitis. While it can infect individuals of all ages, infection rates are particularly high in infants. Globally, approximately 90% of children are infected with RSV before age two. For some, it progresses to severe lower respiratory tract disease, making it a primary cause of infant hospitalizations.Clinical evidence for Abrysvo was secured through the Phase 3 MATISSE study. The results showed that maternal vaccination during late pregnancy significantly reduced the risk of severe RSV-related lower respiratory tract disease in infants within six months of birth.Regarding safety, commonly reported adverse reactions included injection site pain, headache, myalgia, and nausea.Abrysvo is established as a preventive option in major overseas markets. In the U.S., it was approved in 2023 for the prevention of RSV-LRTD in infants via maternal vaccination (32–36 weeks) and for adults aged 60 and older. Last year, the indication was expanded to include adults aged 18 and older.Upcoming competition in RSV prevention strategy for children: Vaccines vs. Antibody InjectionsAntibody therapy, 'Enflonsia (clersrovimab),' for RSV prevention MSD has also entered the infant RSV prevention market.MSD Korea recently submitted an approval application to the Ministry of Food and Drug Safety (MFDS) for 'Enflonsia (clersrovimab),' an RSV preventive antibody injection for neonates and infants. The company anticipates approval by the second half of this year.Unlike vaccines, antibody injections deliver antibodies directly into the body, providing immediate protective effects following administration.Enflonsia is a long-acting monoclonal antibody targeting the F protein. It is designed to maintain preventive efficacy for approximately five months with a single dose, covering the typical RSV season from autumn to the following spring.Notably, Enflonsia was developed as a fixed-dose (105mg) treatment regardless of body weight, which is evaluated as a feature that increases convenience for pediatric prevention programs.In the Phase 2b/3 CLEVER study, a single administration of Enflonsia reduced the incidence of RSV-related LRTD by 60.5% and the risk of RSV-related hospitalization by 84.3%.Furthermore, the Phase 3 SMART study involving high-risk infants confirmed its preventive efficacy and a safety profile similar to 'Synagis (palivizumab),' the existing RSV preventive antibody.Antibody therapy 'Beyfortus' for RSV preventionIf Abrysvo and Enflonsia are approved, they are expected to compete with other long-acting RSV preventive antibodies.Currently, 'Beyfortus (nirsevimab),' an RSV preventive antibody developed by Sanofi, has already entered the infant market.Beyfortus is launching in Korea this year and is garnering attention as a major infant RSV prevention option.Previously, AstraZeneca's Synagis was used for RSV prevention, but its short half-life necessitated multiple doses during the RSV season. In contrast, Beyfortus is a long-acting antibody with an extended half-life, allowing for full-season protection with a single administration.Recent international studies have also compared the effectiveness of these different prevention strategies. A large-scale population-based study in France comparing maternal vaccines and infant antibody strategies found that the Beyfortus group had a lower risk of RSV-related hospitalization.Additionally, a surveillance study conducted in the U.S. showed that Beyfortus was 81% effective in preventing RSV-related hospitalizations, with efficacy maintained for approximately 4 to 7 months. Researchers found that while both strategies reduce RSV-related hospitalizations, antibody-based prophylaxis provided greater protection against severe disease.

- Company
- Leclaza launches in Germany, accelerates Europe entry
- by Cha, Ji-Hyun Mar 13, 2026 09:06am
- Photo of Yuhan Corp’s Leclaza (source: Yuhan Corp)Leclaza, a lung cancer drug developed by Yuhan Corporation, has successfully entered the health insurance reimbursement system in Germany, the largest pharmaceutical market in Europe. This listing is expected to accelerate Leclaza’s entry into other European countries.According to the biotech industry on the 12th, Germany’s Federal Joint Committee (G-BA), responsible for evaluating health insurance reimbursement in Germany, assigned billing codes 761990MO and 761990MP to Leclaza 80 mg and 240 mg, respectively, starting this month. Billing codes are assigned after drug price negotiations are finalized, enabling hospitals to bill health insurance for the medication after prescribing it.Leclaza is a third-generation treatment for non-small cell lung cancer (NSCLC) targeting epidermal growth factor receptor (EGFR) mutations. It received approval in Korea in January 2021 as the country's 31st domestically developed new drug. The combination therapy of Leclaza and Rybrevant received approval from the U.S. Food and Drug Administration (FDA) in August 2024 as a first-line treatment for adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) with confirmed EGFR exon 19 deletion or exon 21 L858R substitution mutation.Later, at the end of 2024, the European Commission (EC) also approved the Lecelaza and Johnson and Johnson’s Rybrevant combination therapy as a first-line treatment for EGFR-mutated NSCLC. Subsequently, in July of last year, the G-BA determined that the combination therapy had sufficient clinical value to qualify for health insurance reimbursement.Under Germany’s Social Code Book V (SGB V), new drugs can enter the market immediately after receiving marketing authorization. Within approximately 6 months, the G-BA evaluates the drug’s clinical benefit, after which price negotiations with health insurers begin. Negotiations typically conclude within another 6 months, after which hospital billing codes are assigned.The G-BA ultimately determined that the combination therapy of Leclaza and Rybrevant positively impacts survival rates for lung cancer patients. It particularly noted a relatively pronounced survival benefit in the patient group aged 65 and under. The G-BA estimated the annual number of patients expected to receive treatment in Germany to be between 1,250 and 3,025.Germany is widely regarded as one of the most stringent countries in Europe in terms of drug pricing decisions. However, Lazertinib entered the reimbursement system relatively smoothly, being recognized for its clinical value. Once prescriptions gain traction in the German market, it is expected to positively influence drug pricing negotiations and insurance listings in other European countries as well.Once sales expand in major European countries, Yuhan Corporation is expected to receive additional licensing fees. Yuhan has not yet received the USD 30 million milestone payment for Leclaza’s approval in Europe. In addition, if sales grow in the European market, the company will receive royalties based on a certain percentage of sales according to the licensing agreement.Yuhan Corporation's total licensing revenue over the 7 years from 2019 to last year amounted to KRW 460 billion. Of this amount, cumulative licensing revenue from Lazertinib technology transfer alone has reached approximately USD 275 million, including upfront payments and development and regulatory milestones.Yuhan Corporation received a non-refundable upfront payment of USD 50 million when it licensed Leclaza to Janssen Biotech, a Johnson & Johnson subsidiary, in November 2018. Subsequently, a USD 35 million milestone was paid in 2020 when the clinical trial for the combination therapy of Rybrevant and Leclaza began. The company received an additional USD 65 million the same year when patient enrollment for the clinical trial began.The company continued to generate milestone revenues thereafter based on progress in development and regulatory approvals. A USD 60 million milestone was triggered by the 2024 U.S. Food and Drug Administration (FDA) approval. Last year, the company received additional milestone payments of USD 15 million for Japanese approval and USD 45 million for Chinese approval.

- Company
- Polivy makes 3rd bid for reimbursement…DREC review imminent
- by Eo, Yun-Ho Mar 13, 2026 09:06am
- Attention is focused on whether Polivy, the first new first-line treatment for diffuse large B-cell lymphoma (DLBCL) in 20 years, will succeed on its third attempt to obtain reimbursement listing in Korea.According to industry sources, Roche Korea's Polivy (polatuzumab vedotin), a treatment for relapsed or refractory diffuse large B-cell lymphoma (DLBCL), is expected to be submitted to the Health Insurance Review and Assessement Service's Drug Reimbursement Evaluation Committee next month (April).It remains to be seen whether progress can be made approximately 8 months after passing the Cancer Disease Deliberation Committee last July.Originally, Polivy sought reimbursement in 2021 for its first approved indication as a third-line therapy, in combination with the BR regimen (bendamustine + rituximab), but the application failed to pass CDDC review at that time.Later, in the first half of 2023, Roche submitted a reimbursement application for first-line therapy using Polivy in combination with R-CHOP therapy (rituximab, cyclophosphamide, doxorubicin, and prednisone). However, this application also failed to pass the Cancer Disease Deliberation Committee in February 2024.Expectations are high for Polivy's latest reimbursement attempt. Roche has submitted additional follow-up analysis results with a 60.9-month follow-up period from the POLARIX study, which evaluated the effectiveness of Polivy in combination with Pola-R-CHP as a first-line treatment for DLBCL.The study, presented at the American Society of Hematology (ASH 2024) annual meeting, has been regarded as the first clinical trial in 20 years to expand the standard first-line treatment for DLBCL. Key results show patients receiving Polivy combination therapy demonstrated a clear improvement in overall survival (OS) compared with those treated with the existing standard therapy, R-CHOP.The lymphoma-related mortality rate was 9.0% in the Polivy combination therapy group and 11.4% in the R-CHOP control group. At approximately 5 years after treatment initiation, the mortality risk in the Polivy combination therapy group decreased by 15%, an improvement over the previous 3-year follow-up result (6% risk reduction).In addition, patients receiving the Polivy combination therapy (38.7%) required follow-up treatments (radiation therapy, systemic chemotherapy, or CAR-T cell therapy) about 25% less frequently than those in the R-CHOP control group (61.7%).Meanwhile, diffuse large B-cell lymphoma (DLBCL) is an aggressive type of blood cancer and the most common form of non-Hodgkin lymphoma. In South Korea, the number of new patients diagnosed with DLBCL is estimated to reach 5,000 each year.Accounting for the highest proportion of non-Hodgkin lymphomas, diffuse large B-cell lymphoma is an aggressive lymphoma requiring immediate treatment due to its rapid progression. Although more than half of patients respond well to treatment and achieve remission, 30–40% of patients either fail to respond to the standard therapy R-CHOP or experience relapse after first-line treatment.Despite the fact that most patients experience relapse within two years and that survival is only about six months upon relapse, making it a highly lethal disease, relapsed/refractory diffuse large B-cell lymphoma remains an area with limited effective treatment options.
- Policy
- Debate over fast-track listing of new drugs continues
- by Jung, Heung-Jun Mar 12, 2026 08:35am
- Debate continues over the proposed reform of the drug pricing system aimed at shortening the reimbursement listing period for new drugs. On one side are calls to strengthen treatment access, while on the other are concerns that the reform could sharply increase the burden on Korea’s national health insurance budget.While working bodies like HIRA are preparing to strengthen post-listing control, concerns persist about the effectiveness and potential side effects of expedited listing.The Korean Pharmacists for Democratic Society, which previously called for reconsideration of the fast-track listing initiative together with the Citizens' Coalition for Economic Justice (CCEJ) last month, plans to hold a briefing session next week to point out issues in the proposed new drug pricing reform.AI-generated imageOn the 10th, the Korea Alliance of Patient Organizations urged the government to promptly implement the fast-track listing and post-listing evaluation system, arguing that delays in national health insurance reimbursement after regulatory approval for anticancer drugs and rare disease treatments are reducing treatment accessibility.The government recently announced that starting in 2026, it will launch a pilot program for a “fast-track listing–post-evaluation system,” which would shorten the reimbursement listing period for rare disease treatments from the current maximum of 240 days to within 100 days. The alliance called for the swift implementation of the measures.KAPO emphasized, “Rather than blocking entry at the early stage, it is important to establish a sophisticated post-listing evaluation and management system based on treatment performance.”Until recently, attention surrounding the drug pricing reform had focused largely on price cuts for already-listed drugs, while the direction of the fast-track listing reform for new drugs received relatively less attention. The pharmaceutical industry, which has little reason to oppose faster market entry, had been cautiously waiting for details of the implementation plan.However, the issue gained prominence in February when groups including CCEJ, the Korean Association for Serious Diseases, and the Korean Pharmacists for Democratic Society urged reexamination of the fast-track listing policy. They also called for a public hearing on issues including raising the ICER threshold and introducing flexible drug pricing agreements.Criticism calling for broader social discussion is expected to continue this month. The Korean Pharmacists for Democratic Society is expected to hold a briefing on March 18 on the proposed new drug pricing reform and express opposition to the fast-track listing policy.An official from the organization said, “Although there are measures to evaluate outcomes and provide refunds if necessary, there are no clear post-management mechanisms, such as price reductions or market withdrawal, after post-evaluation. As the financial burden on the National Health Insurance is expected to surge, preparing countermeasures must be prioritized.”The official continued, “There are also doubts about whether strengthened post-listing management measures are appropriate for Korea. The briefing will address the impact of the overall new drug pricing reform, including fast-track listing.”Critics also argue that the reform of the new drug pricing system, like the proposed price cuts for generics, lacked sufficient prior discussion.A pharmaceutical industry official said, “As with the generic drug pricing reform, this situation arose because sufficient discussion was not conducted before the reform plan was announced. If there had been even a process to coordinate the implementation measures, the current backlash would not have occurred.”
- Company
- Quadrivalent meningococcal vaccine 'MenQuadfi' prescribed at gen hospitals
- by Eo, Yun-Ho Mar 12, 2026 08:35am
- Sanofi Korea's MenQuadfiThe quadrivalent meningococcal vaccine 'MenQuadfi' is now available by prescription at major general hospitals.According to industry sources, Sanofi Korea's MenQuadfi (Meningococcal Polysaccharide Tetanus Toxoid Conjugate Vaccine), indicated for the prevention of invasive meningococcal disease (serogroups A, C, Y, and W), has passed the Drug Committees (DC) of 23 medical institutions nationwide. These include tertiary general hospitals such as Seoul National University Hospital and Asan Medical Center, as well as medical institutions, including Kyung Hee University Hospital at Gangdong, Konkuk University Medical Center, National Medical Center, and Soonchunhyang University Hospital.MenQuadfi was approved in Korea last April, and this drug is given as a single-dose administration in individuals aged 6 weeks to 55 years.Notably, MenQuadfi is the only vaccine in Korea approved with proven efficacy against meningococcal serogroup A in infants aged 6 weeks to less than 24 months. A key feature of the product is its ready-to-use liquid formulation, which eliminates the need for reconstitution or mixing, thereby enhancing convenience for healthcare providers. The immunization schedule consists of four doses for infants aged 6 weeks to less than 6 months, two doses for those aged 6 months to less than 24 months, and a single dose for individuals aged 2 to 55 years.Meningococcal disease has been pointed out as a significant global public health concern. Classified as a Group 2 legal infectious disease with a fatality rate of approximately 10–14%, it affects 500,000 people worldwide annually.Primary symptoms include headache, fever, neck stiffness, vomiting, and altered consciousness, often accompanied by petechiae or purpura fulminans. The importance of prevention is signified by the fact that 11–19% of survivors suffer from long-term sequelae, including hearing loss, cognitive impairment, and neurological disorders.Since meningococcal disease is transmitted via respiratory droplets or direct contact, vaccination is highly recommended for individuals entering communal living environments. Typical candidates include military recruits and first-year college students who plan to live in dormitories.Furthermore, vaccination is advised for travelers or residents in high-incidence areas such as the African meningitis areas, as well as pilgrims traveling to Mecca, Saudi Arabia. Other recommended groups include individuals with immune system disorders, such as complement deficiencies, and those with anatomical or functional asplenia.Meanwhile, in clinical trials, MenQuadfi demonstrated non-inferiority across all four serogroups compared to existing quadrivalent meningococcal vaccines. Specifically, in the 10–55 age group, the seroprotection rates for MenQuadfi were 94.7% in Group A, 95.7% in Group C, 96.2% in Group W, and 98.8% in Group Y.Additionally, studies in children aged 2–9 years confirmed non-inferiority to existing quadrivalent vaccines, with seroprotection rates ranging from 86% to 99%. The vaccine also demonstrated stable immunogenicity when co-administered with other pediatric vaccines.

- Policy
- ‘Active INN prescribing needed for drugs with supply shortages’
- by Jung, Heung-Jun Mar 12, 2026 08:35am
- Han-sook Kim, Director of Health Insurance Policy Division, MOHWThe government said it is reviewing various measures while expressing support for introducing INN (international nonproprietary name) prescribing for drugs with unstable supply.It also stated that it will continue consultations to minimize the impact of the drug pricing reform plan on the field and will further refine the system even after implementation.On the 11th, Han-sook Kim, Director of the Health Insurance Policy Division at MOHW, stated at the National Assembly's drug pricing system discussion forum, " There are many concerns surrounding INN prescribing due to conflicting stakeholder interests. From the perspective of preventing supply instability, it is necessary to actively utilize INN prescribing. We are reviewing various aspects, including the criteria for supply instability and the safety, efficacy, and effectiveness of INN prescribing.”When asked about the direction of the drug pricing reform, Kim said the government would consider the policy’s impact on the field and remain open to consultations and improvements.Director Kim explained, ”The government is also paying close attention to the sustainability of the National Health Insurance finances. We are making multifaceted efforts. Improving unreasonable structures is crucial, and advancing the drug pricing system reforms is part of that effort.“Kim added, “This is an agenda with diverse perspectives. The government cannot clearly predict the impact the reform will have on the field once implemented. The government cannot clearly predict the impact on the field when drug pricing system reforms are implemented. Even after the reform is implemented, we will strengthen monitoring and make improvements if problems arise.”Kim dismissed concerns that the drug pricing reform plan concentrates insurance spending on multinational pharmaceutical companies, and said that it was a misunderstanding.Kim said, “The drug pricing reform could be misunderstood as a policy favorable to the global pharmaceutical industry. But promising companies and technologies must receive investment. If cost savings are generated through the reform, it will be used to properly reward companies investing in R&D.”
- Policy
- Doctors "If INN prescribing is enforced, will boycott the SPD"
- by Kang, Shin-Kook Mar 12, 2026 08:34am
- Doctors who took to the National Assembly to protest the promotion of International Nonproprietary Name (INN) prescribing legislation have said they will go as far as a total boycott of the Separation of Prescribing and Dispensing (SPD) system if the bill is enforced.On the 11th at 4:00 PM, the Korean Medical Association (KMA) Special Committee for public health promotion held a rally in front of the National Assembly Main Building in Yeouido to block the INN prescribing legislation.The doctors gathered at the National Assembly held pickets reading "Will Declare SPD System Annulment if INN Prescribing is Enforced" and demanded an immediate halt to the legislative process.At the scene, Kim Taek-woo, KMA president, emphasized, "INN prescribing is not merely about selecting a chemical component. It is a highly sophisticated professional medical act performed after considering the patient's comprehensive condition. This irrational bill, which prioritizes pharmacy inventory over patient needs when dispensing medication, must be scrapped immediately."The Korean Medical Association (KMA) Special Committee for public health promotion held a rally in front of the National Assembly Main Building in YeouidoKim warned the government and the National Assembly, saying, "Do not trade the public's health for economic logic. While pharmacist groups mislead public opinion by citing ambiguous budget savings, no budget can be more precious than the lives of our citizens."Kim further stressed, "If INN prescribing is enforced, we will regard it as a unilateral breach of the Medical-Pharmaceutical-Government Agreement and declare the total nullification of the SPD system. If our right to prescribe is violated and patient safety is threatened, we will stake everything, including my presidency, on this struggle."Following him, Kim Kyo-woong, Chairman of the KMA representative council, pointed out, "INN prescribing is not simply a systemic change. It is an act that denies the medical judgment of physicians who have precisely diagnosed a patient's condition. Furthermore, it is a highly irresponsible idea that breaks the continuity of treatment and puts patients at risk."Lee Ju-byung, Chairman of the Special Committee to Oppose INN Prescribing, asked, "The new bill states that failure to comply with mandatory INN prescribing will result in up to one year in prison or a fine of up to 10 million KRW. Is this such a serious crime? Who proposed that a doctor should face imprisonment for not prescribing by ingredient name?Lee raised his voice, saying, "Some say doctors prescribe by brand name to receive rebates," adding, "Then, are you advocating for INN prescribing just to receive rebates yourselves?"Lee added, "If the government insists on mandating INN prescribing for the sake of the public, we doctors will, in accordance with the government's will, launch a movement to prescribe only original drugs solely for the benefit of the people."Park Jong-hwan, President of the Medical Association Council for 25 clinics in Seoul, also noted, "On one hand, they say we must implement INN prescribing for public convenience, but on the other hand, they want to forcibly close large-scale pharmacies that the public can use late at night and which offer a wide range of drug choices," adding, "Isn't this an act of inconsistency?"Park stated, "The legislation proposed by Rep. Jang Jong-tae is a self-contradiction," adding, "Both bills contain the words public and patient, but the actual public and patients are nowhere to be found. They only look toward the interests and votes of specific professional interest groups."Park concluded, "I do not know whether it is a National Assembly member's job to pass bills that give all dispensing authority to pharmacists through INN prescribing and protect the interests of small pharmacy owners by regulating large pharmacies, or if this is simply for the benefit of a specific group."

- InterView
- ‘Broader access to CAR-T cell therapy needed for DLBCL’
- by Son, Hyung Min Mar 12, 2026 08:34am
- Diffuse large B-cell lymphoma (DLBCL) is a highly aggressive hematologic malignancy in which a significant number of patients achieve a cure with first-line therapy, but prognosis worsens sharply once relapse or treatment resistance occurs.In particular, patients who relapse or become refractory within 12 months after first-line therapy often struggle to achieve meaningful outcomes with conventional high-dose chemotherapy followed by autologous stem cell transplantation alone. Experts therefore stress the importance of shifting treatment strategies at an earlier stage.Against this backdrop, Gilead’s CAR-T therapy Yescarta (axicabtagene ciloleucel) is emerging as a new alternative based on clinical evidence accumulated in second- and third-line treatment settings.Professor Yun-seok Choi of Seoul St. Mary’s Hospital and Tony Li, Executive Director and Head of Medical Affairs at Kite International Region (Gilead’s oncology subsidiary), emphasized in a recent meeting with Dailypharm, “For DLBCL, the time to relapse and the number of treatment lines directly correlate with prognosis. This is why we must actively consider introducing CAR-T cell therapy at the second-line treatment stage.”Tony Li, Head of Medical Affairs at Kite International Region; Yun-seok Choi, Professor of Hematology-Oncology at Seoul St. Mary’s HospitalDLBCL is the most common subtype of aggressive non-Hodgkin lymphoma. Despite the standard first-line therapy R-CHOP (rituximab, cyclophosphamide, vincristine, prednisone), a substantial number of patients either relapse or become refractory to treatment.The problem is that after just one relapse, treatment response rates and survival prospects decline rapidly. High-dose chemotherapy and autologous hematopoietic stem cell transplantation, which have been the mainstay second-line therapy, require stringent patient selection and still carry a considerable risk of relapse even after treatment.In Korea, Yescarta was approved in August last year for DLBCL and primary mediastinal B-cell lymphoma (PMBCL), and its reimbursement criteria were established in January for third-line treatment by the Cancer Disease Deliberation Committee. However, reimbursement criteria for second-line use in patients who relapse or become refractory within 12 months of first-line therapy have not yet been established.Experts highlight unmet needs in the DLBCL treatment landscape, emphasizing the clinical value of Yescarta and the need for earlier CAR-T introduction in the second-line setting.Q. What are the practical difficulties or limitations of conventional treatments for DLBCL patients who relapse or become refractory after first-line therapy?[Professor Choi] Traditional second-line therapy consists of high-dose chemotherapy followed by autologous stem cell transplantation. However, this approach can only be applied to patients who meet certain conditions, such as being relatively young and having good overall health. Furthermore, relapsed DLBCL is often biologically aggressive, making treatment challenging.[Executive Director Tony Li] Standard first-line regimens like R-CHOP are highly effective, with about 70% of patients achieving a cure. However, treatment becomes increasingly difficult for patients with relapsed or refractory disease. Cure rates inevitably decline with each subsequent treatment line.Stem cell transplantation requires high-dose chemotherapy before the transplant, meaning patients must be in excellent physical condition to endure the entire process. They must be able to withstand the process of receiving anticancer treatment, responding to it, and then undergoing the transplant. Even among patients who successfully undergo transplantation, about 50% eventually relapse, and the prognosis for these patients is not optimistic.Q. In some countries, CAR-T or bispecific antibodies are reimbursed as second-line therapy. What clinical value does Yescarta have in real-world practice?Tony Li[Executive Director Tony Li] Yescarta has been approved in more than 20 countries and is recommended as a Category 1 option for second-line treatment of DLBCL in the National Comprehensive Cancer Network (NCCN) guidelines. This demonstrates that Yescarta has established itself as an evidence-based treatment option in the global clinical setting.Yescarta’s efficacy as a second-line therapy was demonstrated in the ZUMA-7 clinical trial. In this prospective controlled trial comparing Yescarta with standard stem cell transplantation therapy, Yescarta achieved results surpassing the existing standard therapy for the first time in 25 years. The median event-free survival (EFS), the primary endpoint, was 8.3 months in the Yescarta group, representing a significant improvement of approximately four times compared to the 2 months observed in the transplant group.It is also the first and only currently available CAR-T therapy to demonstrate statistically significant overall survival (OS) in a second-line setting.The drug also has accumulated meaningful long-term data. ZUMA-7 has accumulated nearly four years of follow-up data, showing a flattening of the OS curve. In the third-line setting, the 5-year follow-up results from ZUMA-1 confirmed that approximately 43% of patients survived, suggesting the potential for long-term survival.[Professor Choi] DLBCL is a disease with a high likelihood of death if the condition is not adequately controlled in the first line. This is the natural course of DLBCL observed in clinical practice.Even when high-dose chemotherapy followed by autologous stem cell transplantation is performed, the success rate is about 50%, meaning the number of patients rescued by this treatment is limited. In ZUMA-7, the OS curve for the standard-treatment group did not reach a complete plateau.In this context, Yescarta demonstrated statistically significant survival benefits compared to standard treatment, reducing the risk of death. Particularly significant is that CAR-T therapy has, for the first time in the history of DLBCL salvage therapy, presented survival data in a patient population with high mortality risk.Furthermore, the 5-year follow-up analysis of ZUMA-1 reported a 5-year OS estimate of 42.6% for patients treated with Yescarta. This suggests that approximately 4 out of 10 patients can expect long-term survival. Additionally, the fact that Yescarta demonstrated a survival benefit in the second-line setting in the ZUMA-7 study is also significant.Q. In January, reimbursement criteria for third-line Yescarta were established. How might this change third-line treatment strategies?[Professor Choi] Comparing the OS curves, Yescarta's data shows a relatively higher position compared to Kymriah (tisagenlecleucel). Although this was not confirmed through a direct head-to-head trial, many clinicians believe Yescarta may have stronger anti-lymphoma activity, not only in DLBCL but also in follicular lymphoma. This perception could influence drug selection decisions to some extent going forward.Another factor is that Yescarta transports cells to manufacturing facilities without freezing them, which reduces certain regulatory burdens associated with human cell handling permits (such as GMP) required for some CAR-T therapies, potentially enhancing accessibility from the healthcare provider's perspective. This characteristic could also influence future drug selection and market share to some extent.Q. I understand that some countries overseas have approved Yescarta’s reimbursement as a second-line treatment. What are the benefits of using Yescarta in second-line therapy?[Executive Director Tony Lee] In the A8 countries referenced by Korea for drug pricing, Yescarta is reimbursed for both second- and third-line treatments. Clinical study results have consistently shown that using CAR-T therapies at earlier stages is associated with superior treatment outcomes. This trend was reported in studies ranging from ZUMA-1 to ZUMA-7.Additionally, the ZUMA-12 study, which evaluated Yescarta's efficacy in the first-line treatment of LBCL patients, also yielded positive results. The ZUMA-23 study, comparing standard therapy with Yescarta in first-line treatment, is also underway.The healthier the T cells, the higher the likelihood of producing effective CAR-T therapies. This is because patients are less exposed to chemotherapy at earlier stages, meaning their overall condition is likely better, and their immune function is more preserved. These conditions provide the rationale for earlier use of CAR-T therapy, as better treatment outcomes can be expected when CAR-T is administered under such circumstances.Q. Why is reimbursement for Yescarta necessary in second-line treatment?Yun-seok Choi[Professor Choi] Yescarta is a therapy that has demonstrated clinical efficacy in the second-line setting through clinical studies. Based on this evidence, it is evaluated as a meaningful treatment option for clinicians.For immunotherapies that rely on T-cell activation, T-cell fitness is extremely important. While it is challenging to quantitatively assess a patient's T-cell status, this remains an area of ongoing research.Anticancer drugs used in lymphoma treatment are agents that can selectively affect lymphocytes. Therefore, the more a patient is repeatedly exposed to anticancer therapy, the more the fitness of the patient's T cells, which serve as the material for CAR-T, or the patient's own T cells that should attack cancer cells when dual-specific antibodies are administered, inevitably decreases.Considering this, T-cell–based immunotherapy should ideally be introduced earlier, when immune function is still relatively preserved. Applying CAR-T therapy under normal immune conditions can yield better treatment outcomes, offering advantages in terms of long-term patient prognosis and quality of life.Reimbursement decisions should also consider treatment outcomes rather than focusing solely on drug prices. Patients who responded well in the ZUMA-1 and ZUMA-7 studies were able to return to daily life and resume economic activity. Given the unique disease course and therapeutic innovation in DLBCL, reimbursement decisions should proceed more quickly.Q. With the emergence of various new drugs like bispecific antibodies and early-stage CAR-T cell therapy, treatment options have broadened. Specifically, what are the criteria for patient groups where early-stage CAR-T therapy is deemed more urgent and suitable than conventional standard therapy?[Professor Choi] Patients at the second-line treatment stage, particularly cases where patients relapse within 12 months after first-line therapy. Through large-scale clinical trials, only Yescarta demonstrated effective results in patients who relapse or become refractory within 12 months after first-line treatment. It is the sole option with an approved indication for this patient group. Bispecific antibodies currently lack prospective evidence focused specifically on this patient population.However, CAR-T is not an immediately available treatment, requiring turnaround time (TAT).Should evidence for bispecific antibodies accumulate in the future, making both options available, clinicians will need to carefully consider treatment strategies. A cautious approach is warranted, weighing CAR-T's TAT against the biological aggressiveness of DLBCL in the relapse patient population and the rationale for bispecific antibodies in this setting.Q: What insights do you believe the global experience accumulated with Yescarta could provide for the domestic treatment environment?[Executive Director Tony Lee] The approval of Yescarta as a third-line therapy in Korea is a significant advancement, which can serve as a starting point that can open new treatment opportunities for both patients and healthcare providers. As experience with Yescarta accumulates in the third-line setting, we expect Korean healthcare providers' understanding of the drug's efficacy and characteristics to deepen.In addition, real-world data (RWD) continue to accumulate globally, and this evidence may support future discussions on second-line reimbursement in Korea. Given that approval and reimbursement have already been granted in several countries, we anticipate that discussions in Korea will also proceed based on an evaluation of the drug's clinical value.Q. How do you expect the DLBCL treatment landscape to evolve?[Professor Choi] About 70% of DLBCL patients can expect cure, but the remaining 30% fall into a high-risk group. Future research will likely focus on more precise identification of high-risk patients and tailored treatment strategies based on risk level.In particular, we anticipate a shift where T-cell-based immunotherapies, such as CAR-T, move to earlier treatment lines and are introduced earlier for high-risk patients.