- LOGIN
- MemberShip
- 2026-04-29 05:11:03

- Policy
- Reimbursement application submitted for 'Adempas tab'
- by Lee, Tak-Sun Jul 10, 2024 05:48am
- Bayer’s Bayer’s 'Adempas tab,' a treatment for chronic thromboembolic pulmonary hypertension (CTEPH), is being considered for reimbursement listing 10 years after its approval as a novel drug. According to industry sources on July 2nd, a reimbursement decision application for Adempas was recently submitted to the Health Insurance Review and Assessment Service (HIRA). This drug obtained approval in South Korea as an orphan drug in June 2014. Five products with different doses are available, and it has the efficacy and the effect in ▲patients with persistent/recurrent chronic-thromboembolic pulmonary hypertension (CTEPH, WHO Group 4) after surgical treatment or inoperable CTEPH, to improve exercise capacity ▲adult patients with arterial pulmonary hypertension (PAH, WHO Group 1) who have WHO functional class 2-3, to improve exercise capacity. Adempas has been known as the first novel drug to treat CTEPH. CTEPH occurs in patients with chronic pulmonary embolism who progress to chronic obstructive pulmonary disease (COPD) and develop fibrotic stenosis and occlusion, leading to pathological vascular remodeling and increased resistance in the pulmonary arteries. CTEPH is a chronic disease that causes progressive shortness of breath and right heart failure. Symptoms include dyspnea, fatigue, chest pain, dizziness, peripheral edema, cough, and hemoptysis, significantly impacting quality of life. Ultimately, it can progress to heart, kidney, and liver failure, potentially leading to death. Treatment options include pulmonary endarterectomy (PEA) surgery. However, 40% of patients are ineligible for surgery, making drug therapy crucial. Therefore, Adempas was highly anticipated to be the first drug. It has been 10 years since it was approved in South Korea. However, patients had high economic burden because the drug was not covered by the National Health Insurance reimbursement. The industry attributes the drug’s case to the low drug price. According to IQVIA, the drug’s sales performances for the past five years remain at zero. However, Bayer applied for reimbursement 10 years after obtaining the approval. "In clinical trials, Adempas improved symptoms and occurrence rate in CTEPH patients, and it also demonstrated an effect in alleviating shortness of breath," a Bayer representative said. "When the drug becomes reimbursement listed, it will significantly help patients."

- Policy
- 1st bispecific antibody Epkinly approved with a condition
- by Lee, Hye-Kyung Jul 09, 2024 05:51am
- 'Epkinly (epcoritamab),' the first T-cell–engaging bispecific antibody, was found to have been approved under the condition that the company submits Phase III trial data. In Korea, the approval was granted on March 20 based on Phase II clinical trial data and a Phase III trial protocol, but at the time, a condition was added that the company must submit data from a therapeutic confirmatory trial. According to the minutes of the Central Pharmaceutical Affairs Committee meeting held in April, which were recently released by the Ministry of Food and Drug Safety, Epkinly was granted conditional approval and was required to submit Phase III trial results after the approval of the product by applying Article 24, Paragraph 3 of the 'Regulations for Approval and Review of Biological Products, etc. 'Epkinly (epcoritamab),’ which is imported by Abbvie Korea, is a bispecific monoclonal antibody that binds to both the CD3 on the surface of T-cells and CD20 on the surface of B-cells and is indicated for the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) after 2 or more lines of systemic therapy In Korea, Polivy, Kymriah, Selinexor, and Columvi are approved for the treatment of patients with relapsed or refractory DLBCL. DLBCL is one of the most common blood cancers and is one of the most common types of widely spread (diffuse) non-Hodgkin lymphoma, characterized by rapid progression. Epkinly binds to CD3 to activate T cells and binds to CD20 to bring B cells to the side of activated T cells and induce B cell death. In this regard, a CPAC member said, "In a clinical trial in patients with persistent relapses requiring 3 or more cycles of treatment, Epkinly demonstrated some degree of effectiveness and safety. Its effectiveness and safety have been confirmed over other existing drugs, so we deemed granting conditional marketing authorization was appropriate pending the results of its Phase III clinical trial." When the U.S. FDA granted the drug through its accelerated approval program, the approval was based on the Phase I/II EPCORE NHL-1 study. In 148 patients with relapsed or refractory DLBCL who had received a median of 3 prior therapies, the drug demonstrated an objective response rate of 61%, a complete response rate of 38%, and a median duration of response of 15.6 months in patients with CD20-positive diffuse large B-cell lymphoma. Another CPAC member added, "Based on the Phase II results, Epkinly appears to be an effective and safe agent when compared to other 2nd or later line agents. Therefore, we believed the conditional approval was warranted, subject to submission of its Phase III results."
- Policy
- BMS’ Camzyos and Handok’s Empaveli pass the DREC review
- by Lee, Tak-Sun Jul 09, 2024 05:51am
- Bristol Myers Squibb Korea’s 'Camzyos Cap,' a treatment for symptomatic obstructive hypertrophic cardiomyopathy (oHCM), has passed the Drug Reimbursement Evaluation Committee (DREC) review after reconsideration. Handok’s 'Empaveli Inj,' a treatment for paroxysmal nocturnal hemoglobinuria (PNH), also obtained approval for reimbursement and moved on to negotiations. The Health Insurance Review and Assessment Service (HIRA) commenced the 7th Drug Reimbursement Evaluation Committee (DREC) of 2024 and announced that it had decided the appropriateness of reimbursement for these drugs. The review outcome of assessing the appropriateness of benefit coverage for drugs that have applied for a decision: Three pharmaceuticals have been considered for this round of DREC review. The symptomatic oHCM treatment, Camzyos Cap, a PNH treatment, Empaveli Inj, and an NMOSD treatment, Uplizna Inj, received the assessment. Among these, Camzyos Cap and Empaveli Inj obtained appropriateness of reimbursement decisions. Two drugs are expected to undergo drug pricing negotiations with the HIRA and will receive the final decision for reimbursement listings. Camzyos received the reconsideration decision from the DREC review held last month. In just one month, DREC granted the reimbursement appropriateness. On the other hand, Uplizna Inj received a decision that it will meet the appropriateness of reimbursement if the company accepts an amount below the standard. If Mitsubishi Tanabe Pharma accepts an amount below the standard, the drug will be considered for negotiations with the HIRA. If the company fails to take it, the drug will not be listed for reimbursement. If the company accepts an amount below the standard for exemption from the drug pricing negotiations, it will only negotiate the expected claim amount.
- Policy
- Reassessing the comparison of foreign drug pricing is 'idle'
- by Lee, Tak-Sun Jul 08, 2024 05:46am
- The 10th public-private meeting has been held to reassess the comparative methods of foreign drug pricing. However, they exchanged different opinions without reaching a concrete decision. Pharmaceutical industry has particularly opposed to the use of drug pricing references from Germany and Canada. It remains to be seen how the two parties will continue the discussion regarding this matter. According to industry sources, the 10th meeting to reassess the comparative methods of referencing foreign drug pricing was held on the morning of July 5th. The government initially planned to convene the meeting in June, planning to complete gathering opinions, but due to schedule delays, the meeting took place in July. This indicates that the government has considered the current meeting as the final round of gathering opinions. However, the pharmaceutical industry, the attendee of the meeting, argues that further discussion is needed. The differences in opinions are in the reference drug pricing in Germany and Canada, which the government compares drug prices to. The Korean government advocates public reimbursement prices as the reference, while the pharmaceutical industry argues for sales prices. They argued strongly about this matter during the current meeting. The industry argues that comparing Korean drug prices by referencing the public reimbursement price in Germany and Canada, which are also implementing reference-pricing systems, will distort the differences in drug pricing. Under those countries’ reference-pricing systems, China and India’s low-priced generics are frequently reimbursed. The industry argues that the government’s current comparison method works against its aim to set a reasonable drug price by making comparisons to advanced countries (A8). The meeting confirmed the differences in opinions of the government and the industry. Therefore, it remains to be seen whether there will be a next meeting. Since the government claims to have gathered enough feedback, it will likely maintain its current position. Drug pricing is anticipated to be set this year by implementing a weighted mean price comparison method, excluding the highest and lowest drug prices of A8 countries, every three years. It will be applied to pharmaceuticals for chronic diseases that expect patent expirations. The government is likely to pursue the current drug pricing reference sources. However, the two parties are likely to communicate privately until the government makes an official announcement. As a result, the final proposal may change.

- Policy
- 10th external reference pricing reeval meeting is held
- by Lee, Tak-Sun Jul 05, 2024 05:48am
- The 10th meeting for the external reference pricing reevaluations is scheduled to be held this Friday (July 5). The meeting, which was scheduled to be held on June 27th, has been postponed to this week. The meeting between the government and the pharmaceutical industry, which has been held since November last year, is being held for the 10th time this time. It will be interesting to see if the two sides will be able to conclude their talks through this 10th meeting. According to industry sources on the 3rd, the 10th meeting on the reevaluation of foreign drug prices is scheduled for the 5th. The government and the pharmaceutical industry will be meeting after a month since the 9th round of talks that was held on the 10th of last month. At the 9th meeting, the government reportedly expressed its intention to end the discussions. It said that it had gathered enough opinions over the 8 months of talks. However, the pharmaceutical industry believes that the matter requires further discussion, as well as the postponement of the external reference pricing reevaluations. On how to compare the price, which was the most controversial issue, the plan to compare the weighted average of the A8 (Japan, France, Germany, Italy, Switzerland, the United Kingdom, Canada, and the United States) countries’ insurance ceiling price after excluding the highest and lowest price with Korea’s insurance ceiling price, is likely to become the set option. The government notified the industry of this approach at the 8th meeting, and a similar approach was used in the recently concluded research service as well. The industry is concerned that the domestic price ceiling will be higher than that of the external reference price if the formula excludes the U.S., where generic prices are high, resulting in a large price cut. They are opposing the government's proposal due to this, but since it is unlikely that the plan will be withdrawn, they are focusing on revising the remaining details. In particular, the government and the industry have different opinions on the sources of referencing the drug price. The government is using publicly available drug prices in Germany and Canada, but the industry is arguing to base the pharmaceutical manufacturer’s selling price. Also, the industry requested the sum price of the single drugs be ensured for combination drugs. However, the government holds all the cards in the discussion. The industry believes that the government is likely to hasten the external reference pricing reevaluations as a way to save money, as it has recently invested additional health insurance finances to expand medical school admissions. A pharmaceutical industry official said, “I don't understand the government's logic for reducing domestic generic drug prices through the external reference pricing system when even Switzerland, a pharmaceutical powerhouse, has recently raised generic drug prices due to supply instability.”

- Policy
- Daewoong·Ildong late entries to the dapagliflozin market
- by Lee, Tak-Sun Jul 04, 2024 05:52am
- Daewoong Pharmaceutical and Ildong Pharmaceutical have made late entries in the market for diabetes treatment containing 'dapagliflozin.' Although the door to the biosimilar market for dapagliflozin opened in April last year, these two companies did not join the market immediately. It was presumed because of the contract binding with AstraZeneca, which owns the original product. After resolving the binding contract and with Forxiga’s imminent withdrawal from the Korean market, two companies have likely entered the competition for the market. According to industry sources on July 3rd, Daewoong Pharmaceutical’s 'Forxilo Tab 10 mg (dapagliflozin propanediol hydrate)' and Ildong Pharmaceutical’s two products of 'Daformet SR Tab (dapagliflozin bis L-proline/metformin hydrochloride)' became listed for reimbursement as of July 1st. Forxilo Tab is a generic version of Forxiga (AstraZeneca), the original monotherapy, and Daformet SR Tab is a biosimilar referencing Xigduo XR tab (AstraZeneca) with a change to the salt form. As the substance patent for dapagliflozin expired on April 7th, most pharmaceutical companies in South Korea have released either generics or biosimilars, such as salt-form-changed products. However, Daewoong and Ildong were the exceptions. At the time, Daewoong was in a joint agreement with AstraZeneca to sell Forxiga and Xigduo. Ildong was preparing to launch reimbursed 'Qtern,' a combination therapy containing dapagliflozin plus saxagliptin. Because of the joint-sales agreement with AstraZeneca for Qtern, Ildong could not release biosimilar referencing Forxiga and Xigduo. Two companies entered the market for biosimilars as Forxiga was set to withdraw from South Korea after the canceling approval in April, and Xigduo’s joint-sales agreement was transferred to HK inno.N instead of Daewoong Pharmaceutical from January. Daewoong Pharmaceutical listed 'Forxilo Tab 5 mg,' acquired through a transfer and acquisition deal, for reimbursement in April. This month, Daewoong Pharmaceutical joined the competition in the market with reimbursed Forxilo Tab 10 mg, acquired through a transfer and acquisition deal. Daewoong Pharmaceutical and Ildong Pharmaceutical join the market for biosimilars referencing Forxiga or Xigduo. Daewoong Pharmaceutical has six years of experience selling the original Forxiga, from 2018 until last year. Its generic drug is expected to settle in the market quickly. Furthermore, Daewoong Pharmaceutical is also preparing to obtain reimbursement for its biosimilar, “Forxilomat SR tab (dapagliflozin·metformin hydrochloride).” The company is expected to launch biosimilars soon. Ildong Pharmaceutical launched the reimbursable 'Dafor Tab 10 mg (dapagliflozin bis L-proline),' a biosimilar containing a salt form change, and secured reimbursement for its combination therapy. The company is expected to pursue sales and marketing of its products. As major pharmaceutical companies, Daewoong Pharmaceutical and Ildong Pharmaceutical, enter the market despite their one-year delay, the competition among biosimilars is expected to intensify.

- Policy
- GSK will discontinue supply of Infanrix IPV
- by Lee, Tak-Sun Jul 02, 2024 05:48am
- GlaxoSmithKline has decided to discontinue supply of its ‘Infanrix IPV’ vaccine, which protects against diphtheria, tetanus, pertussis, and polio in children, in South Korea. Infanrix IPV and Sanofi Pasteur's ‘Tetraxim’ are the only DTaP-IPV vaccines used in the National Immunization Program (NIP), raising concerns about the shortage of vaccines and the shortage of vaccinations that will follow. GSK reported to the MFDS that it will discontinue the supply of Infanrix IPV Prefilled Syringe as of July 1. The reason for the suspension is low domestic demand. The company said, "It is difficult to import additional supply, and it will not be possible for the company to participate in future NIPs after the stock is exhausted. The remaining stock is expected to run out in January next year. In fact, sales of Infanrix IPV on IQVIA last year were not captured. Tetraxim, on the other hand, generated sales of $3.1 billion. The vaccine is used to prevent diphtheria, tetanus, pertussis (whooping cough), and polio in infants and children from 2 months of age. It is administered as 3 intramuscular injections of 0.5 mL at 2, 4, and 6 months of age, followed by a booster dose of 0.5 mL at 4 to 6 years of age. Infanrix IPV has experienced pediatric immunization shortages in the past. In 2016, the global DTaP vaccine shortage disrupted pediatric immunizations due to domestic supply disruptions. In 2016, a global shortage of the DTaP vaccine disrupted pediatric immunization schedules, and when the domestic supply of Infanrix IPV was temporarily suspended, Tetraxim’s stock also ran out due to high demand. In 2021, GSK’s vaccine was also suspended due to a paperwork error, and the MFDS allowed cross-immunization with an alternative vaccine. Such history suggests that the discontinuation of Infanrix IPV in the Korean market will inevitably cause disruptions on-site. A fundamental solution for this is localizing pediatric vaccines. Recently, LG Chem has begun localizing a hexavalent combination vaccine for infants and young children, but it will take time for the product to be commercialized in Korea. An industry official said, “Vaccines for nationally mandated vaccinations such as DTaP are entirely imported from foreign countries. Localization of vaccines required for nationally mandated vaccinations is urgently needed to protect people's health and improve national competitivity as seen during the COVID-19 crisis." .
- Policy
- Expenses for the major four severe diseases tops KRW 7T
- by Lee, Tak-Sun Jul 01, 2024 05:47am
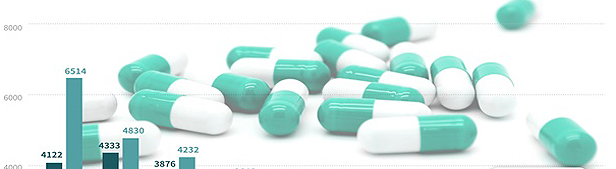
- Pharmaceutical expenses for the four major severe diseases exceeded KRW 7 trillion last year. The four major severe diseases refer to cancer diseases, cerebrovascular disease, and rare·severe incurable diseases. Pharmaceutical expenses for this category have risen due to high-cost pharamceuticals. Consequently, an analysis suggests that managing pharmaceuticals in this category is crucial for continuing the National Health Insurance. The Health Insurance Review and Assessment Service (HIRA) published the '2023 Report on Reimbursement Claims for Pharmaceuticals Expenses' on June 27th. It indicates that the claim amount for the four major severe diseases last year was KRW 7.348 trillion, a 20% increase from KRW 5.8495 trillion in 2022. Pharmaceutical expenses for the four major severe diseases (unit: 1,000 cases, KRW 1 million). Notably, pharmaceutical expenses for cancer disease and rare·severe incurable diseases are increasing rapidly. Anticancer drug expenses have reached KRW 4 trillion. Last year’s expense was KRW 3.8506 trillion, up 23.5% Year-over-Year (YOY). Pharmaceutical expenses for rare·severe incurable diseases topped KRW 3 trillion. It was KRW 3.337 trillion for 2023, up 16.2% YoY. Pharmaceutical expenses for cerebrovascular and cardiac diseases were KRW 803.5 billion and KRW 700.5 billion, respectively, and they have maintained an increasing trend. In contrast, the percentage of pharmaceutical expenses out of the total medical fees for the National Health Insurance has remained at 23% for the past two years. Last year’s figure was 23.86%, an increase from 23.34% in 2022 but still at around 23%. From 2019 to 2021, pharmaceutical expense was at around 24%. However, last year’s rate of increase in pharmaceutical expenses showed the highest figure in the past five years. The rate of increase for pharmaceutical expenses was 12%, recording a double-digit figure. This seems to be relevant to the rapid increase in pharmaceutical expenses for the four major severe diseases. Last year’s total pharmaceutical expense was KRW 25.6446 trillion. The percentage of pharmaceutical expense for the major four severe diseases out of the total expense amounted to 27.4%. The government is in the process of improving the post-management system and re-assessment for pharmaceutical expense management. Specifically, it plans to establish a system to post-manage high-cost pharmaceuticals after reimbursement and re-assess the pricing, such as lowering the pricing after comparing to foreign drugs or patent-expired drug costs.

- Policy
- Gov't releases generic drug price comparison study results
- by Lee, Tak-Sun Jun 27, 2024 05:47am
- The government's decision to fully disclose the 'Study on Measures to Improve the Generic Drug Pricing System,' which ended in April, ahead of the final meeting for the external reference pricing reevaluations, is being analyzed as a sign that the authorities intend to push ahead its plan to cut generic drug price through reevaluations. In particular, the industry believes the government is using media to publicize the study findings that the generic drug price is up to 10 times more expensive in Korea than in other countries, excluding the U.S., as a means to justify the reevaluation. According to industry sources on the 25th, the 10th meeting on the external reference pricing reevaluations is scheduled for the 27th. The government is reportedly planning to finalize the process of collecting opinions from the pharmaceutical industry within this month. Therefore, the 10th meeting is expected to be the final meeting between the government and the industry. In this situation, there are voices that the recently released study on how to improve the generic drug pricing system is just the government’s means to justify its plan for external reference pricing reevaluations. The study compared drug prices with the A7 countries (Canada, France, Germany, Italy, Japan, Switzerland, and the United Kingdom), excluding the United States, where generic prices are relatively high. As a result, as of 2022, the price of hyperlipidemia generics in most countries was 0.09 to 0.41 times cheaper than those in Korea. However, the study concluded that the comparison of Korean generic drug prices with those of A8 countries showed differences by efficacy group and API and that there is a limit to unilaterally applying price cuts to generic drugs. The pharmaceutical industry analyzes that the comparison of drug prices excluding the U.S. used in the study is similar to the recent government's proposed external reference pricing reevaluation, which suggested using an adjusted average price that excludes the highest and lowest prices among the A8 countries. This is because excluding the highest price removes the U.S. price, which has the highest generic drug prices, from the comparison. As shown in the study, excluding the U.S. price will lead to Korea having relatively high prices for hyperlipidemia drugs, and domestic pharmaceutical companies are concerned that the performance of related generic drugs will suffer from the price cuts that may follow. An industry official said, "Off-patent drugs can become cheaper abroad than in Korea over time. In foreign countries, generics occupy a higher market share than the original over time, so they can maintain sales even at the lowered price." On the other hand, the industry official explained that there is no difference between Korea and the A8 countries when comparing generics that newly entered the market upon patent expiry. "It is problematic to compare overall prices based on only one aspect when generic prices vary depending on the time of launch or disease. We should be giving incentives to increase the generic drugs’ market share and grow the market pie like foreign countries." The study also proposed the creation of a market structure that allows generic drugs to gain competitiveness. For example, in order to create a drug pricing structure where drug prices can be reduced over time after generics enter the market, it is necessary to strengthen not only the pricing policies used at the time of drug listing but also policies to encourage the use of low-priced products in the field. However, the government will likely first focus on lowering domestic generic prices through external reference pricing system.
- Policy
- Some Akynzeo products recalled due to insufficient API
- by Lee, Hye-Kyung Jun 27, 2024 05:47am
- The Ministry of Food and Drug Safety (MFDS) recalled some lot numbers of HK Inno.N's antiemetic ‘Akynzeo Cap’ after confirming the possibility that the drug may not contain enough active pharmaceutical ingredient (API). On the 21st, the MFDS issued a recall order for Akynzeo batch number '43000563 [2026-11-30].’ The reason for the recall was the possibility of the drug lacking some of its API (palonosetron hydrochloride). HK Inno.N also informed wholesalers of the voluntary recall of Akynzeo and asked them to send the drug back to the warehouses of companies that have the affected product. HK Inno.N imported Akynzeo from the Swiss pharmaceutical company Helsinn. It is indicated for the prevention of initial nausea and vomiting or the prevention of acute and delayed nausea and vomiting induced by repeated treatment in adults receiving moderate emetogenic cancer chemotherapy. It contains fosnetupitant (as chloride hydrochloride) and palonosetron hydrochloride, which work by inhibiting neural pathways involved in nausea and vomiting. Both ingredients have a long plasma half-life, making them effective antiemetic agents.