- LOGIN
- MemberShip
- 2026-06-10 18:16:27

- Policy
- Changes to Price-Volume Agreement (PVA) negotiation guidelines
- by Jung, Heung-Jun May 12, 2026 11:30am
- The scope of drugs eligible for one-time rebate contracts as an alternative to permanent price cuts during Price-Volume Agreement (PVA) negotiations will be expanded.Under the government's policy to address low birth rates, drugs reported increased use due to expanded coverage for infertility procedures will now be eligible for one-time rebate agreements.When medicines from national stockpiles are deployed to respond to legal infectious diseases, they will be included in the list of drugs excluded from PVA negotiations. On the 11th, according to industry sources, the National Health Insurance Service (NHIS) is collecting opinions on the draft amendment to the "Detailed Operating Guidelines for Price-Volume Agreement Negotiations" until this afternoon.The NHIS aims to clarify the targets for one-time rebates, which serve as an alternative to price cuts, and expand their scope by establishing new criteria.As these regulations were originally introduced in response to COVID-19, the targets have been clarified as follows ▲Cases where a production/import request or administrative action from related agencies is confirmed for responding to an infectious disease at the 'Caution' level or higher of the crisis alert ▲Cases where it is confirmed through related agencies that an unavoidable supply disruption or shortage occurred for the sole alternative to the negotiated drug during the year preceding the analysis period due to issues with production facilities or raw material supply.Furthermore, a new clause has been established for cases where the use of drugs under 'infertility procedure reimbursement standards' has increased due to expanded policy support, such as changes to reimbursement criteria.Inclusion in these categories does not automatically mandate a one-time rebate contract. The new regulation also allows for the adjustment of the negotiation reference price for one-time rebate targets.Regarding drugs excluded from negotiations, drugs under a Risk Sharing Agreement (RSA) will be removed from the exclusion list. Drugs used as state-stockpiled materials to respond to legal infectious diseases will be added.For ingredients classified as national stockpiled materials under the Act on the Prevention and Control of Infectious Diseases, any usage of these stockpiled drugs for legal infectious disease response will result in an exclusion from PVA negotiations.In contrast, considering the purpose of the RSA, which is to share the uncertainty of the impact on insurance finances, relevant drugs will no longer be eligible for exclusion from negotiations.The definition of 'voluntary price reduction,' which qualifies a drug for exclusion from negotiations, will also be clarified. Currently, items where the 'reduction rate through voluntary application is greater than the reduction rate according to the negotiation reference price' are excluded from negotiations.However, this will be restricted so that voluntary price reductions resulting from evaluation outcomes, such as reimbursement adequacy re-evaluations or prior price cuts for reimbursement expansion, or those following specific contract terms with the NHIS do not qualify for exclusion.The updated PVA negotiation guidelines containing these details will be implemented following the opinion-gathering period and will apply starting with drugs currently undergoing monitoring or negotiation.
- Policy
- Middle East war crisis accelerate regulatory flexibility
- by Lee, Jeong-Hwan May 12, 2026 11:30am
- Amid the government’s push to address gaps in regional, essential, and public healthcare, the prolonged Middle East conflict is accelerating efforts to ease regulatory barriers through AI and telemedicine.The Ministry of Health and Welfare plans to take the lead in advancing regulatory reforms to fully utilize new medical technologies, such as AI and telemedicine, in order to strengthen regional, essential, and public healthcare and respond to the crisis caused by the war in the Middle East.The Ministry has already begun implementing measures to directly deliver medical supplies, such as syringes, IV sets, and medications, via telemedicine to patients with rare and intractable diseases, who are facing even greater difficulties in securing medical supplies due to the war in the Middle East.On the 9th, the Ministry announced plans to explore regulatory rationalization measures that would allow for the aggressive use of AI and telemedicine as part of efforts to strengthen regional, essential, and public healthcare.Currently, the Ministry is in the final stages of administrative procedures to establish a Regional, Essential, and Public Healthcare Division (hereinafter referred to as the “REPH Division”). Following consultations with the Ministry of the Interior and Safety, a consensus has been reached on the necessity of establishing the division, and efforts to secure the necessary personnel and budget are currently underway.Based on the establishment of the REPH Division and organizational restructuring, the Ministry of Health and Welfare intends to identify additional measures to integrate new medical technologies into regional, essential, and public healthcare.A prime example is the Primary Care Innovation Pilot Project, an initiative where local governments and regional primary care institutions design policies to proactively reform regional, essential, and public healthcare and submit them to the Ministry of Health and Welfare. Upon review, the Ministry provides policy and budgetary support.In particular, as the government is now able to respond to public health needs through dedicated public health officials based on the supplementary budget passed by the National Assembly, it will identify additional cases of regulatory exemptions for AI and telemedicine.An example of such a regulatory exemption is the collaboration between the Ministry of Health and Welfare and the telemedicine platform SolDoc to allow the direct delivery of medical supplies via telemedicine, aimed at minimizing the impact on patients with rare and intractable diseases caused by the fallout from the Middle East war.The Ministry of Health and Welfare has already begun administering the direct delivery of medical supplies to patients with rare diseases using a qualification verification system linked to SolDoc and medical institutions.These supplies, which include syringes, IV sets, suction tips, suction catheters, sterile saline, and disinfectant swabs, are essential for the home treatment of patients with rare diseases. The Ministry plans to gradually expand this in stages to include the delivery of medications as needed.With the passage of the revised Medical Service Act by the National Assembly, telemedicine will be fully institutionalized starting this December. The main provisions of the law include broadly permitting telemedicine for patients with rare diseases and allowing hospitals and higher-level medical institutions to provide telemedicine services under certain restrictions.The Ministry of Health and Welfare plans to expand telemedicine services based on regional, essential, and public healthcare until the Telemedicine Act takes effect.A Ministry official explained, “Since addressing gaps in regional, essential, and public healthcare is a key policy direction for the Ministry, we will develop additional measures to strengthen regional, essential, and public healthcare using AI and telemedicine, alongside the establishment of the new REPH Division.”A medical industry official also noted, “Following efforts to strengthen regional, essential, and public healthcare, and the prolonged Middle East war, the Ministry of Health and Welfare has repeatedly shown signs of seeking to relax healthcare regulations through telemedicine and new AI technologies. We are closely monitoring the situation, as there have been some instances where sufficient consultation with healthcare counterparts has not been conducted under the pretext of regulatory exemptions.”

- Policy
- Review initiated on introducing 'indication-based drug pricing'
- by Jung, Heung-Jun May 11, 2026 09:18am
- The National Health Insurance Service (NHIS) is proceeding with a fiscal impact review for the introduction of an indication-based pricing system. The final decision on whether to implement the system is expected to be determined by the results of this research.In March, the Health Insurance Policy Review Committee (HIPRC) decided to review the feasibility and effectiveness of indication-based pricing. Consequently, the NHIS has initiated follow-up measures by commissioning a research project.According to the NHIS on the 8th, a public bid has been announced for a research project titled “Analysis of Indication-Based Drug Price Evaluation Status and Feasibility Review Study,” which is to be completed by the end of this year. The research is scheduled to run for 5 months following contract signing, with a planned completion date between November and December.The NHIS plans to finalize the research project related to the of indication-based pricing system by November or December. There have been consistent criticisms that the current single-price operation of the national health insurance system has limitations in adequately reflecting the value of innovative new drugs for severe and rare diseases.Through this study, the NHIS will analyze the benefits and effects of improved accessibility under an IBP system, as well as the limitations and costs associated with allocating the health insurance budget. The research findings will serve as a reference for future policy decisions.The contents of the research consists of ▲Literature review of previous domestic and international studies related to IBP ▲Current status of IBP operations in major overseas countries ▲Objective measurement and analysis of patient accessibility benefits and fiscal impacts for multi-indication drugs ▲Opinion surveys and in-depth interviews with the public, academia, the pharmaceutical industry, and the government ▲Comprehensive policy recommendations for system improvement.Specifically, the NHIS plans to evaluate fiscal impacts through drug price simulations for each indication. The study will also cover the types of drugs to be included in the system, reimbursement evaluation, drug price calculation methods, and mechanisms for post-reimbursement expenditure management.Furthermore, the NHIS will examine the overall aspects of the indication-based pricing system, including its pros and cons, operational points of contention, and policy considerations.The NHIS anticipates that "We will derive mid-to-long-term development directions for the 'expansion of scope of use' system based on the categorization of reimbursement expansion for multi-indication drugs."The research results are planned for use in establishing a mid- to long-term roadmap for creating an innovative new drug ecosystem and in informing government policy decisions.The research schedule includes an interim report meeting in September~October and a final report meeting in October~November. The research is scheduled for completion at the end of the year.

- Policy
- Inheritance of drug price ceiling to be blocked in transfers
- by Jung, Heung-Jun May 08, 2026 01:15pm
- Changes are expected to the current rules that allow drug price ceilings to be inherited during product transfers. The system is likely to revert to past regulations that apply the lower of the new calculated price and the price at the time of transfer.As a result, acquiring high-priced generics to avoid the impact of drug pricing reform will no longer be viable.According to industry sources on the 6th, a working-level consultative body comprising the Ministry of Health and Welfare and industry representatives recently discussed changes to the transfer regulations that were not brought before the Health Insurance Policy Deliberation Committee in March.The rules governing price ceilings in transfers have changed multiple times. Until 2020, prices were set based on the lower of the final ceiling price of the transferred product and the newly calculated price.However, following the stepwise pricing reform, industry backlash arose as transfers were treated as new listings, leading to significant price drops.In response, the government allowed inheritance of the existing ceiling price starting during transfers in 2021.Now, the government plans to revert to the previous rule, applying the lower of the existing ceiling and the new calculated price.Even if a high-priced generic is acquired, the newly calculated price at the moment of transfer is applied, effectively enforcing a lowest price rule.Pharmaceutical companies that had considered acquiring high-priced generics to avoid pricing reform will lose this option.With the reform, the generic pricing rate has been reduced to 45%, and the reduction rate for products failing to meet the baseline requirements has been strengthened from 85% to 85%. Combined with multi-listing management rules, prices could fall to as low as 30.6% within one year if bioequivalence studies are not conducted.Previously, companies might have chosen to acquire products with higher maintained prices.However, if prices are reset based on the calculation price at the time of transfer, transfers that take existing drug prices into account become meaningless.
- Policy
- Innovative pharmas need permanent pricing incentives
- by Lee, Jeong-Hwan May 08, 2026 01:15pm
- Rep. In-soon Nam of the Democratic Party of Korea has drawn attention by stating that permanent pricing incentives for innovative pharmaceutical companies should be institutionalized in order to advance Korea into a pharmaceutical and biotech powerhouse and create blockbuster new drugs.Rep. Nam criticized the Ministry of Health and Welfare, noting that while the ministry recently formalized a differential drug pricing system between innovative and non-innovative pharmaceutical companies through a resolution by the Health Insurance Policy Deliberation Committee, the inclusion of preferential pricing for innovative pharmaceutical companies only as a temporary provision left some gaps.Regarding legislation to introduce limited international nonproprietary name (INN) prescribing, Rep. Nam also expressed the view that it would be reasonable to either remove penalty provisions for doctors who fail to comply with mandatory INN prescribing regulations or to downgrade and relax these penalties to administrative fines.Her point is that policy and legislation should be pursued with a focus on ensuring that the public can access frequently out-of-stock and essential medicines without barriers, setting aside conflicts between specific professions such as doctors and pharmacists.Having officially announced her candidacy for Deputy Speaker of the second half of the 22nd National Assembly, Rep. Nam In-soon promised that, if elected, she would strive to create a national environment that advances the pharmaceutical and biotech industry and enhances public access to essential medicines.On the 7th, Rep. Nam held a meeting with the press corps and stated, “As the Jae-myung Lee administration has adopted a national agenda to transform Korea into a leader in digital health and the pharma-biotech industry, I will consider various ways to support this goal as Deputy Speaker.”“Pharma-biotech lost priority under Yoon administration… will restore momentum”Rep Nam assessed that while fostering the pharma-biotech industry has always been a priority across administrations, interest declined under the former Yoon, weakening growth momentum.In contrast, she noted that the Lee administration has set a goal of becoming one of the world’s top 5 pharma powerhouses and developing domestic blockbuster drugs, raising expectations for policy reforms across related ministries, including the Ministry of Health and Welfare.She therefore argued for the need to permanently extend preferential drug pricing for innovative pharmaceutical companies with the goal of fostering blockbuster new drugs.Rep Nam stated, “I have consistently advocated for differential pricing between innovative and general pharmaceutical companies, and I welcome its inclusion in the recent reform. However, making the incentive temporary limits its impact on new drug R&D investment.”“The government’s goal is to improve the domestic pharmaceutical industry’s structure using the funds secured through drug price cuts. If we want innovative new drugs and blockbusters to emerge in Korea, preferential treatment for innovative pharmaceutical companies cannot be temporary. Instead of offering temporary preferential treatment to innovative companies, we must remove the ‘temporary’ qualifier to allow for active support.”Rep Nam also noted that the Health and Welfare Minister Eun-Kyeong Jeong has shown a strong commitment to fostering domestic new drug development.She said, “The Lee administration has declared its intention to nurture blockbuster drug companies and has merged the Bio Committee and Bio-Health Innovation Committee. Previously, the Ministry of Health and Welfare did not appear to take a leading role, but after speaking with Minister Jeong Eun-kyung following the integration of the innovation committees, it appears the Ministry intends to take the initiative and carry out its duties. The atmosphere will change going forward.”He noted, “Currently, South Korea lags behind advanced countries in terms of pharmaceutical technology, new drug development, and medical AI, so we must catch up quickly. Since I enacted the Special Act on the Promotion of the Pharmaceutical Industry, preferential measures have been stalled for several years. If elected Deputy Speaker, I will prioritize this area in my legislative work.”“Let’s carry out limited INN prescribing focused on patients, without provisions punishing doctors”Regarding the limited INN prescribing bill currently pending in the National Assembly’s Health and Welfare Committee, Rep Nam expressed the view that even if provisions punishing doctors who violate the mandatory generic prescribing requirement are removed, a legislative environment must be created that ensures patients can access essential medicines without inconvenience.She emphasized that, since limited INN prescribing is a key policy agenda item of the current administration, efforts should focus on addressing resistance from the medical community and ensuring smooth institutional adoption.The current bill mandates INN prescribing for selected drugs designated by the Ministry of Health and Welfare following a government committee review, and stipulates penalties of up to one year in prison or a fine of up to KRW 10 million for violations.Rep Nam clearly stated that these penalty provisions should either be removed entirely or downgraded to administrative fines.She also noted the need to carefully consider concerns raised by the Korean Medical Association regarding the scope of bioequivalence testing and trust in substitution and INN prescribing.Rep Nam said, “The KMA is opposing the measure, raising concerns about the broad scope of bioequivalence testing, and their arguments should be taken seriously. We need further discussion on how to incorporate these concerns into policy. For now, it seems there is a lack of objective data or research on generic substitution and INN prescribing, so we need to accumulate more data.”She added, “Gradual implementation of INN prescribing for out-of-stock and essential medicines could serve as a middle ground between physicians and pharmacists. “Public awareness of generic substitution and INN prescribing has significantly increased during the COVID-19 pandemic, as more people have experienced receiving alternative drugs with the same active ingredient.”Nam emphasized, “We should activate systems such as post-notification of substitution and build more research data to support future legislative discussions. But imposing criminal penalties for INN prescribing violations is inappropriate. A more reasonable approach would be to remove penalties or reduce them to administrative fines, prioritize patient-centered legislation, and consider enforcement measures in stages.”“Warehouse pharmacy regulations need to prevent misuse”The recent amendment to the Pharmaceutical Affairs Act, which strengthens regulations on warehouse-style pharmacy advertising, is also one of Nam’s achievements.She explained that the ultimate goal of the regulation is to prevent excessive consumption and misuse of medicines that could lead to adverse effects.The provision in the Pharmaceutical Affairs Act prohibits expressions that may encourage misuse and delegates authority to the Ministry of Health and Welfare to specify concrete and unique expressions that cannot be used in pharmacy names or promotional slogans through subordinate regulations, prioritizing public safety above all else.Rep Nam said, “We also brought forward the implementation date from six months to three months after the government’s promulgation, and added a supplementary provision allowing public health centers to provide administrative guidance to pharmacists opening new pharmacies before the law takes effect. I was the one who codified the provision for pharmacists to provide medication guidance within the Pharmaceutical Affairs Act. At first, pharmacists weren’t very fond of it, but today, medication guidance has become a crucial system and phrase for ensuring public medication safety.”She continued, “When I look at warehouse-style pharmacies, I'm sorry whether pharmacists can actually provide proper medication guidance to patients. We must prevent the public from perceiving medications as mere commodities. Even after my election as Deputy Speaker, I will engage in policy monitoring to curb the misuse of medications by the public by regulating warehouse-style pharmacies.”
- Policy
- MFDS to revise labeling for 951 metformin products
- by Lee, Tak-Sun May 07, 2026 10:29am
- AI-generated imageThe government is pushing to revise the labeling for 951 metformin-containing products, the most widely used diabetes treatment in the market. This measure aims to explicitly state the potentially fatal side effects that may occur when metformin-containing products are administered to patients with hereditary mitochondrial disorders.According to industry sources on the 5th, the Ministry of Food and Drug Safety (Division of Drug Safety Evaluation) recently prepared a proposal to amend the approval conditions based on the European Medicines Agency (EMA)’s safety review regarding metformin-containing products and has begun collecting industry feedback.The key change is to restrict use and require immediate discontinuation in patients suspected or diagnosed with mitochondrial disorders.Under the proposed revision, metformin is not recommended for patients with ▲ MELAS syndrome (mitochondrial encephalopathy with lactic acidosis and stroke-like episodes) and ▲ MIDD (maternally inherited diabetes and deafness), due to increased risks of lactic acidosis and neurological complications.Additionally, if symptoms suggestive of MELAS or MIDD occur after administration, treatment should be immediately discontinued, and prompt diagnostic evaluation should be performed. The analysis indicates that metformin can affect intracellular mitochondrial metabolism, potentially causing severe energy metabolism disorders in patients with underlying genetic diseasesThe revision applies to a total of 951 products, including both monotherapy and combination drugs. As metformin is a core component of the domestic diabetes treatment market, most major pharmaceutical companies, including Chong Kun Dang, Daewoong, Hanmi, and Yuhan, are expected to be affected.The MFDS will accept feedback from relevant associations and companies until May 15. It will then comprehensively review the submitted comments and issue a final order to amend the approved product information.An MFDS official stated, “This measure aims to enhance the safe use of medicines for patients in Korea based on the latest safety information from the EMA. We ask that relevant associations and their member companies submit their review comments within the deadline.”

- Policy
- Government support for the next Leclaza discovery continues
- by Lee, Jeong-Hwan May 06, 2026 03:29pm
- Kang-seop Lim, Director of the Pharmaceutical Bio Industry Division, MOHW“A new drug candidate from the biotech venture Genosco was licensed out to Johnson & Johnson in the U.S. via the mid-sized pharmaceutical company Yuhan Corporation, leading to the creation of Leclaza. This is a prime example of a successful pharmaceutical and biotech startup from Korea. We plan to continue pushing forward with government policies this year to provide full support until the end, ensuring that more startup models emerge, with policies that support the commercialization of such early-stage discoveries.”The Ministry of Health and Welfare is unveiling a specialized startup fostering roadmap for the pharmaceutical and biotech sector for the first time in history, aiming to create domestic blockbuster drugs like a “second Leclaza” from the venture stage.The plan will provide full-cycle support to ensure promising drug candidates are not lost, linking technologies from universities, hospitals, and research institutes to startups, scaling them up, and supporting global expansion.On the 3rd, Kang-seop Lim, Director of the Pharmaceutical Bio Industry Division, stated that a startup support plan will be developed jointly with the Ministry of SMEs and Startups (MSS) and announced by June or July.With the newly established division within MOHW and Director Lim dedicating his full efforts as its first head, there is a growing momentum to develop multifaceted policies for the promotion of the pharmaceutical and biotechnology industry.This initiative follows President Jae-myung Lee’s ‘Startup Nation’ strategy announced in January.At that time, President Lee instructed all government ministries to build a startup ecosystem where anyone, including young people, regional entrepreneurs, and deep-tech startups, can pursue entrepreneurship.The MOHW is joining forces with the MSS on the plan, following their earlier announcement of collaborative measures for pharmaceutical and biotech industry policies.This amounts to establishing specific policy measures to promote and foster startups in the pharmaceutical and biotech industry, with the revitalization of startups in this sector serving as the policy goal and overarching framework.Director Lim pointed to research institutes within universities, medical institution research centers, including those in university hospitals, and government-funded research institutes as the specific targets of this policy.This administrative initiative aims to increase the number of cases where new drug candidates currently being researched by professors, doctors, and scholars are brought to the forefront through government-supported startups, commercialized and productized through processes such as licensing out, and then expanded beyond the domestic market into the global market.Director Lim cited Leclaza as a representative example. He explained that this is a policy in which the MOHW and MSS joined forces to ensure that a highly marketable domestic new drug, capable of succeeding in both domestic and overseas markets, was developed through the Genosco-Yuhan Corporation-Johnson & Johnson track.Director Lim stated, “Lecraza is a representative success case in which an early-stage drug candidate developed by Genosco was licensed by the mid-sized pharmaceutical company Yuhan, and later out-licensed to Johnson & Johnson for commercialization in overseas markets. This is a prime example of a successful pharmaceutical and biotech startup, and the government plans to support more cases like this.”He added, “In Korea, pharma-biotech startups typically emerge through several routes, including ventures founded by professors and researchers in university labs, physicians in hospitals, and researchers at government-funded institutes. A significant number of new drug candidates are likely to originate at the researcher or academic stage. The policy focus is on how the government can support these efforts when they transition into pharma-biotech startups.”Lim continued, “Given the limited size of the domestic market, global expansion is inevitable. We will support pharma-biotech startups not only in scaling up after their establishment, but also through to global expansion and commercialization.”He further stated, “This is the first time the Ministry of Health and Welfare has introduced a policy specifically targeting pharma-biotech venture startups. While we are still working through the details and identifying actionable support measures, we plan to finalize and announce the startup support plan by July. Ultimately, our goal is to establish a Ministry of Health and Welfare policy that identifies and supports startups that will serve as the seeds for large-scale innovative drug development.”

- Policy
- Remote delivery of medical supplies for rare disease patients allowed
- by Lee, Jeong-Hwan May 06, 2026 03:29pm
- Minister Eun-kyeong Jeong ㅆhe Ministry of Health and Welfare announced that starting on the 4th, it will implement a “non-face-to-face direct delivery service for medical products” targeting rare disease patients, patients with severe intractable diseases, and severely ill children.This is to ensure stable access to medical products for patients with rare diseases who are facing difficulties in securing necessary medical supplies due to the prolonged Middle East conflict.Target conditions include short bowel syndrome, Cornelia de Lange syndrome, Pompe disease, and biliary atresia. Medical products (including pharmaceuticals and medical devices) in high demand for each disease group, such as syringes and IV lines, are included in the remote delivery program.The Ministry will provide one-stop support through the telemedicine platform ‘Soldoc,’ which allows patients to consult with representatives via chat and make product purchases and delivery after patients and caregivers go through the verification process.In the future, the model will expand to include customized in-person and remote care, collaboration between large and local hospitals, and delivery of pharmaceuticals and medical supplies.On the 3rd, Minister Eun-kyeong Jeong held a roundtable meeting at Seoul National University Hospital Rare Disease Center with representatives from the Korean Organization for Rare Diseases, SNUH medical staff, and the Soldoc platform to discuss the initiative.During the meeting, participants shared challenges faced by rare disease patients due to the Middle East conflict, and decided to immediately launch a direct delivery service for medical supplies in collaboration with the telemedicine platform Soldoc.Patients with rare diseases are defined as those suffering from rare conditions affecting 20,000 people or fewer, as stipulated by the Rare Disease Management Act. Among these patients, those who must manage their conditions at home using medical supplies such as syringes and IV sets are facing difficulties due to rising prices and shortages of medical supplies caused by the war in the Middle East.In fact, Mr. A, a caregiver for a patient with short bowel syndrome, expressed his anxiety, saying, “I was worried because the IV sets I used to buy online were often out of stock due to the situation in the Middle East.”Ms. B, who cares for a child with Cornelia de Lange syndrome, also said, “Syringes and disposable vials are essential for the children’s nutritional support (enteral feeding) and medication administration, so I was worried I wouldn’t be able to obtain the supplies I usually buy from online shopping sites.”Ultimately, the difficulties in securing medical supplies purchased through online shopping sites due to the fallout from the Middle East conflict led to a partnership between the Ministry of Health and Welfare and the telemedicine platform SolDoc.Unlike general online shopping sites, Soldoc has a system in place to verify eligibility, being linked with medical institutions to confirm whether a patient has a rare disease.Through this system, when a patient with a rare disease or their caregiver submits a purchase request via the internet or app, eligibility verification is easily conducted through the National Health Insurance Service system.Once verified, they can purchase products and receive delivery, paying out-of-pocket for non-reimbursed items.For items covered under medical expense reimbursement that require prescriptions, patients can consult doctors via telemedicine before purchase. Claims are handled by the provider, and patients only pay their coinsured share.Items available include syringes, infusion sets, suction tips, suction catheters, sterile saline, and disinfectant swabs.The Ministry plans to expand the program to include patients with severe intractable diseases and children receiving medical expense support, if necessary.Additionally, the Ministry is considering pharmaceutical delivery for urgent cases.Telemedicine will be formally implemented in December, following revisions to the Medical Service Act. The revised law allows telemedicine for rare disease patients.In particular, patients with rare diseases can receive telemedicine services even at hospital-level or higher medical institutions, and the delivery of drugs and supplies is also permitted. The Ministry plans to strengthen services focused on those requiring essential medical services through telemedicine before the law takes effect.Minister Eun-kyeong Jeong promised, “The state and society will take responsibility to ensure that patients are not marginalized or left in anxiety simply because their diseases are rare. We will provide financial support for the cost of medical supplies if needed after reviewing the burden of medical supply costs.”Meanwhile, on the same day, Minister Jeong, Soon-heon Kwak, Director General of Health and Medical Policy, Jin-hyang Jeong, Secretary General of the Korean Organization for Rare Diseases, seven patients, and six medical staff members, including Joong-shin Park, Vice President for Medical Services at Seoul National University Hospital, held a staff meeting at Seoul National University Hospital in Jongno-gu, Seoul, after the roundtable meeting.
- Policy
- Incrementally modified drugs unaffected by price reform
- by Jung, Heung-Jun May 06, 2026 03:28pm
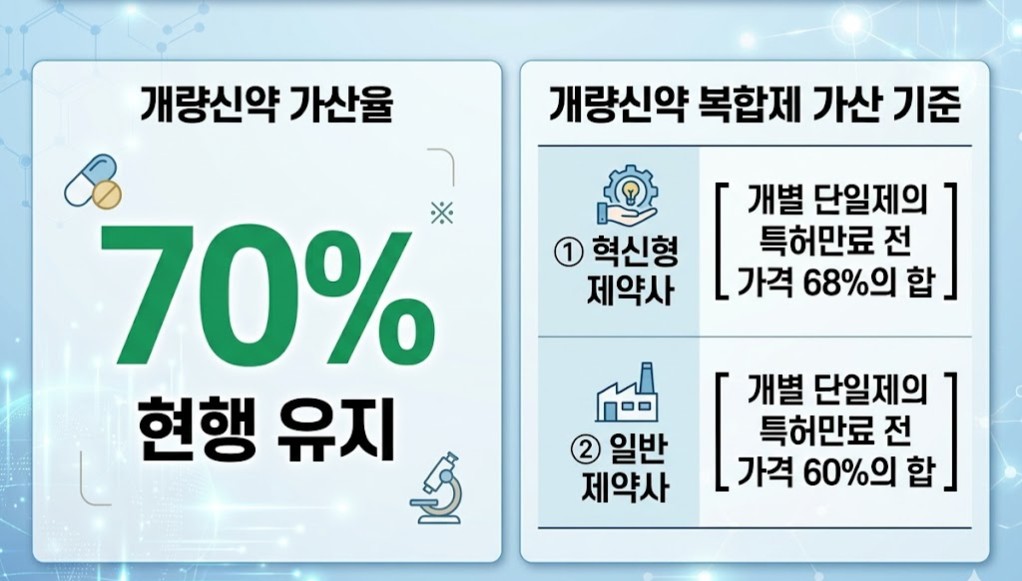
- Under the government’s drug pricing system reform, the insurance pricing premium rates for incrementally modified drugs and their combination products are expected to remain unchanged. Only some conditions related to the duration of the premium are likely to be adjusted.As the pricing calculation rate for generics is set to drop to 45%, domestic companies are expected to show greater interest in developing incrementally modified drugs.According to industry sources on the 6th, during working-level discussions between the government and the pharmaceutical industry, a consensus was reached not to lower the premium for incrementally modified new drugs.Although maintaining the current premium was discussed at the Health Insurance Policy Deliberation Committee (HIPDC) in November last year, the point was excluded from the reform plan approved by the HIPDC in March this year.This led to concerns within the industry that the premium might also be reduced along with the lower pricing calculation rate. There were concerns that lowering the premium could eliminate incentives for R&D investment.Under the current pricing system, incrementally modified drugs receive a premium on a base pricing rate of 53.55%, resulting in a final price of 70%. For new dosage or administration forms, a 58.9% premium is applied, resulting in a price of 77%.For incrementally modified combination drugs, pricing is calculated as the sum of pre-patent-expiry prices of each component. Innovative pharmaceutical companies receive 68% of that sum, while general pharmaceutical companies receive 59.5%.The government is not expected to significantly adjust these premium rates. Instead, it is reported that the preferential premium rate for combination drugs by general pharmaceutical companies—currently a 59.5% sum—will be slightly adjusted to a 60% sum.As the generic pricing rate is reduced from 53.55% to 45% while the incrementally modified drug premium remains unchanged, the price gap between generics and modified drugs is expected to widen further.The conditions for the premium duration are expected to be simplified. Previously, a one-year premium could be extended in two-year increments through conditional approvals and reviews.Going forward, a basic one-year premium will be granted, with an additional three-year extension if domestic manufacturing criteria are met. If no follow-on generics are listed thereafter, the premium may continue.Modified drugs and their combination products that are domestically produced and face no market competition will be able to maintain their premium drug prices for a long time.
- Policy
- What's the reason behind domestically developed CAR-T 'Rimqarto' obtaining Phase 3 waiver?
- by Lee, Tak-Sun May 04, 2026 10:33am
- CAR-T therapy Rimqarto (source: Curocell)Rimqarto (anbalcabtagene autoleucel, Curocell), the first domestically developed CAR-T therapy to be approved in South Korea, has been granted a waiver for Phase 3 clinical trials.This decision is interpreted as the result of a comprehensive consideration of the unique characteristics of the drug as a third-line treatment for lymphoma, as well as the ethical dilemmas associated with comparative clinical trials against existing therapies.According to the results of the Ministry of Food and Drug Safety (MFDS)'s Central Pharmaceutical Affairs Advisory Committee (CPAC) meeting held on April 2, it was concluded that it is appropriate to waive the Phase 3 clinical trial for the new CAR-T (Chimeric Antigen Receptor T-cell) therapy 'Rimqarto' and replace it with post-marketing surveillance.CPAC members highlighted that while Rimqarto has the same basic mechanism as existing CAR-T agents, it introduces a novel mechanism that simultaneously inhibits PD-1 and TIGIT to prevent T-cell exhaustion.According to a recently disclosed meeting report, one member highly evaluated the product's efficacy, stating, "The response rates were better than the clinical results of previously approved therapies, particularly with a high proportion of patients achieving complete remission (CR) and encouraging long-term survival results."Regarding safety, no specific issues were found besides the adverse events typically reported in similar agents (such as CRS and ICANS), and deaths during the trial were judged to have a low correlation with the drug.On the highly debated issue of giving a 'conditional pass for Phase 3 clinical trials,' the committee reached a consensus that it is "practically impossible." First, they viewed it as lacking ethical validity. Given that already-proven CAR-T products are approved and in use, administering a less effective control drug to patients was deemed unethical.The difficulty of patient recruitment was also considered. The patient population in the third-line lymphoma treatment phase has a low survival rate and a small number of candidates, making it extremely difficult to conduct large-scale confirmatory trials that include a control group. Consequently, the CPAC concluded that it is more rational to continuously verify safety and efficacy using Real-World Data (RWD) collected in clinical settings or Post-Marketing Surveillance (PMS), rather than mandating a Phase 3 trial.Based on this CPAC advisory, the MFDS finalized the approval conditions for Rimqarto. The committee agreed that the "product approval is appropriate, given that it is a third-line lymphoma treatment," and decided to disclose the meeting report anonymously.This decision served as a stepping stone toward the rapid supply of an independently developed domestic CAR-T therapy to the field. It is expected to provide new treatment opportunities for patients with severe hematologic cancers who do not respond to existing treatments.Meanwhile, 'Rimqarto Inj' is an orphan drug for the treatment of adult patients with diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma (PMBCL) that is relapsed or refractory after two or more systemic therapies.Rimqarto works by inserting genetic information into the patient's immune cells (T-cells) to enable them to recognize CD19, a surface antigen on B-cells, and then re-injecting these cells into the patient's body to identify and destroy cancer cells expressing CD19. It is designed to inhibit the expression of immune checkpoint receptors PD-1 and TIGIT, thereby blocking cancer cells' immune evasion and inducing enhanced, sustained T-cell responses to increase anti-tumor effects.