“Reimb standard for hemophilia should align with approvals"
The Korean Society of Hematology requests an amendment
Jung, Sae-Im 기자 2023-04-14 05:50:37
Submitted an amendment proposal for hemophilia drugs to the Health Insurance Review and Assessment Service
Single administration dose to be set at the same level as indicated
Will increase the frequency of administration to provide personalized prevention and maintenance therapy for each patient

▲ Young-Sil Park, Treasurer of KSH
Young-Sil Park, Treasurer of KSH (Department of Pediatrics, Kyung Hee University School of Medicine), met with reporters on the 13th and said “We have submitted a proposal for the amendment of the reimbursement standards for hemophilia drugs in the Fall last year and is awaiting results. Although there are several steps left to final reimbursement extensions, I heard that HIRA has shown a positive response."
The amendment to the reimbursement standards that KSH proposed can largely be divided into two parts. Increasing dose amount and frequency of administration. Currently, the reimbursement standard is set narrower than the approved maximum dose and number of administrations. For this reason, it has been pointed out that the treatment effect may be reduced due to insufficient single dosage amount depending on the patient. Therefore, KSH’s argument is that the maximum level in the reimbursement standard should be set at the same level as each drug’s indication.
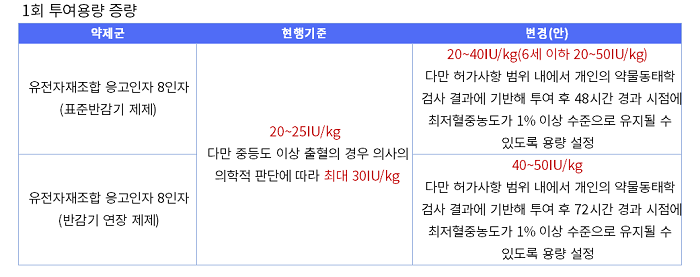
▲ Drug reimbursement standard improvement plan, reconstituted by Dailypharm
Specifically, KSH requested the dosage allowed for administration with each reimbursement to be increased from the current 20-25 (IU/kg) to a maximum of 50. The amendment would allow the dose to be increased flexibly according to the patient's condition, with the dose for standard half-life formulations to range from 20 to 40 (20 to 50 for children under 6 years of age) and extended half-life formulations to range from 40 to 50. These are the scope of dosages specified in the label for each formulation.
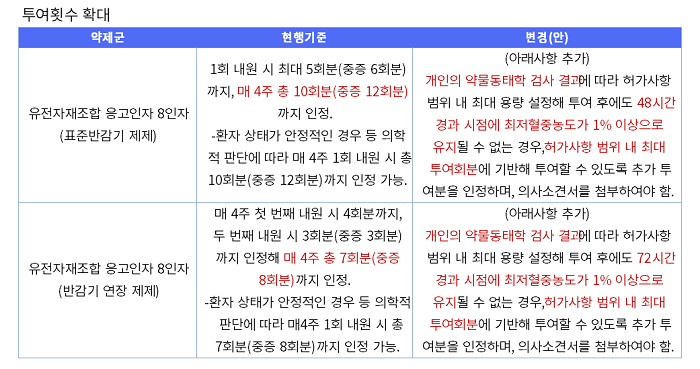
The KSH also suggested the reimbursed number of monthly administrations allowed for patients should be expanded. According to the current reimbursement standard, patients can visit the hospital once or twice a month and receive a total of 10 doses of standard half-life treatments. Severely ill patients are allowed up to 12 doses. A total of 7 doses (8 doses for severely ill patients) are reimbursed for extended half-life drugs during the 1-2 visits per month.
▲ Drug reimbursement standard improvement plan, reconstituted by Dailypharm
This means that standard half-life drugs can be administered three times a week for severe patients. However, experts pointed out that it is often necessary to adjust the frequency of administration depending on the patient's condition. Accordingly, the proposed amendment stipulates that 'if the trough concentration level cannot be maintained at 1% or higher 48 hours after setting and administering the maximum dose allowed according to the individual pharmacokinetic test result, administration of an additional dose up to the maximum dose permitted in the label may be accepted.’
Treasurer Park said, “Currently, patients are administered treatments three times every 7 days, on Day 2, Day 4, and Day 7. In some cases, almost no clotting factors remain in the body on the third day for some patients. Our proposed improvement to the plan offers an increased number of administrations so that the optimal effect can be achieved for those whose minimum coagulation factor level is not maintained on the second day.”
The KSH is requesting another revision 4 years after the reimbursement standards for hemophilia treatment were revised because the hemophilia treatment has now been expanded to maintenance and preventive therapies.
In the past, treatment of hemophilia was centered around ‘replacment therapy', in which clotting factors were administered when bleeding occurred. In recent years, the treatment paradigm has evolved to 'maintenance and prevention therapy', which prevents bleeding in advance by regularly administering clotting factors even without bleeding events. Furthermore, ‘personalized treatment', where a patient’s administration cycle and dose are customized in consideration of the patient's symptoms, living environment, and pharmacokinetics, has emerged as a trend. Currently, the treatment goals for patients with severe hemophilia consist of maintenance and prophylaxis therapies.
Also, the introduction of drugs with extended half-life has reduced the required number of regular administrations, and an application that allows patients to determine their pharmacokinetic levels has been introduced, customized maintenance and prevention therapy have settled as the standard of care.
However, the reimbursement standards that have been set in the past are narrower than the scope approved, which limits the realization of customized maintenance and prevention therapy.
Park added, “The reimbursement standards for hemophilia have improved a lot compared to the past. I believe that a change in the reimbursement standard is necessary to achieve the optimal effect for patients in line with the changes made to the domestic treatment environment and the hemophilia treatment environment. I look forward to the government's positive decision that can allow personalized treatment for each individual in consideration of each patient’s factors."
Jung, Sae-Im 기자 (same@dailypharm.com)